


سوزن گیر اپل apple
نام وسیله : سوزن گیر apple
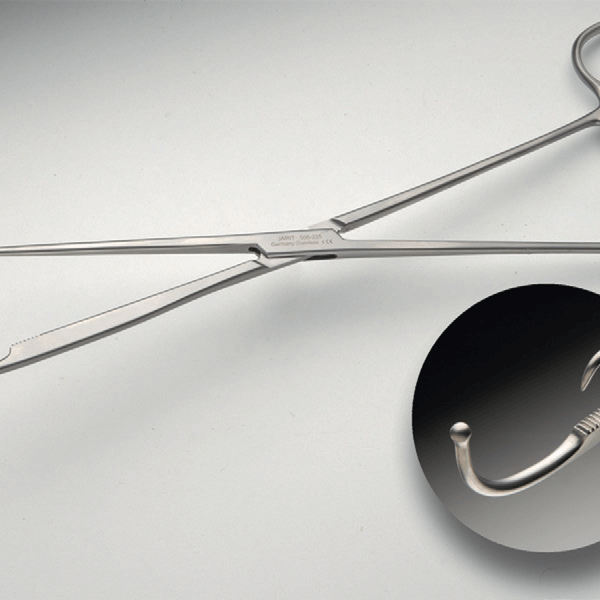
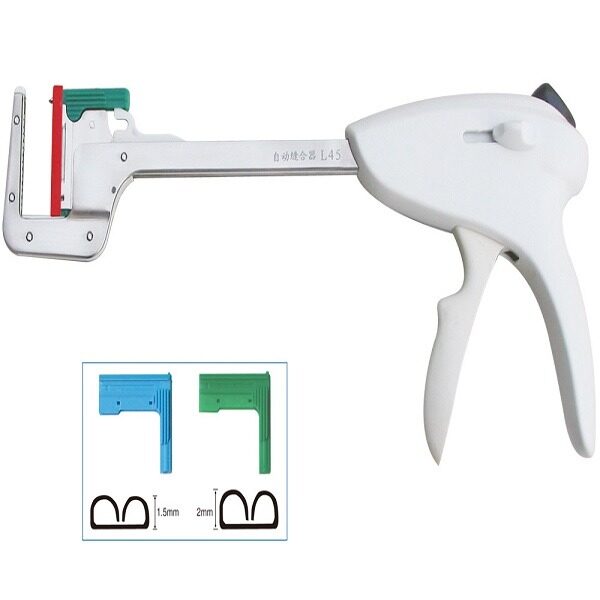
سوزن گیر apple : دارای نوک مستقیم ، کرو و زاویه دار است که سطح داخلی آرواره های آن دارای پوششی کربنی باشیارهای ضربدری میباشد . دسته عملکرد ارتجاعی داشته که رها کردن و بستن آرواره های آن را تسهیل می کند.
مورد استفاده سوزن گیر apple : جهت گرفتن محکم سوزن در حین بخیه زدن کار برد دارد .
برای مشاهده ی صفحه ی اینستاگرام ما می توانید بر روی این لینک کلیک نمایید.
برای مشاهده و خرید انواع ابزار های جراحی عمومی می توانید بر روی این لینک کلیک نمائید .

apple
برای مشاهده محصولات دیگر برروی کلمه ی “ورودبه سایت“ کلیک نمایید./
-Click on the “Login to site“ to view other products. /
Equipment in Laparoscopic Surgery
سوزن گیر اپل apple
Equipment in Laparoscopic Surgery
Helder Ferreira, Carlos Ferreira
Before a new instrument is used, the surgeon should know and test it. It is always better to test
a device before a procedure than during it!
IntroductIon
Over the last 30 years, laparoscopic procedures have
become standard in most surgical diseases.
The rise of
abdominal and pelvic laparoscopic surgery has been a true
revolution in medical practice.
The concept of minimally
invasive approach, with all its advantages such as quicker
recovery, shorter hospital stay and a far superior aesthetic
results has been gaining more and more supporters among
the international surgical community.
The old paradigm
that a big incision meant a big surgeon has dramatically
changed.
The equipment and instruments for performing these
minimally access procedures has, over the years, greatly
improved.
Following the surgeons’ demands, the increasing
investment and research on better tools have provided
more sophisticated and efficient equipment that offers
lower risk and thus higher safety to our patients.
An organized and well-equipped operating room is
essential for successful laparoscopy.
The surgical team
and the operating room staff should be familiar with the
instruments and their functions.
If they are not aware of
an instrument’s mechanism of action, it can interfere with
surgery progression, increasing not only risks for patients
but also surgeon’s anxiety and fatigue. Each instrument
should be inspected periodically.
Scissors, graspers,
trocars, trocar sleeves are checked for loose or broken tips,
even if the same instruments were used during a previous
procedure.
One of the most
important benefits of laparoscopy is the
magnified vision offered by the optics and high definition
cameras and thus better identifies anatomical structures
and dissection plans.
This improved image often permits
a more precise surgical gesture, better hemostasis and
probably less postoperative adhesions.
Almost all instruments available for laparotomy are
now available in a specialized form for laparoscopy.
Instruments and devices that are used in laparoscopy
include the laparoscope (camera), trocars and port devices,
instruments for dissection, hemostasis and ultrasound.
Laparoscopic instruments attempt to reproduce the effects
of conventional laparotomic instruments: Grasping,
dissecting, cutting and coagulation.
LAPAroScoPY VErSuS oPEn SurGErY
Operative laparoscopy requires an advanced degree of
technical skills and training.
The smaller size incisions and
instruments implicate a huge degree of precision only dealt
by imaging systems of high magnification.
In spite of the same final objective, we have to
distinguish the laparoscopic field from the open surgery
ield. Contrary to open surgery where surgeons have a direct
view and manually manipulate and palpate tissues during
the operation, the challenge in laparoscopy is the absence
of stereoscopic vision and the need of transpositioning the
movement of surgeons’ hand through a long small diameter
trocar creating one or more output functions at the distal
part of body cavity.
Some of the specificities of laparoscopic surgery are:
Limited field of vision controlled by an assistant:
Surgeons need an increased cognitive and physical
load to perform the surgery (i.e. the instruments may
intermittently disappear from the surgeon’s vision while
manipulating structures).
Reduced depth perception:
The monitors used in
laparoscopic surgery filter three-dimensional cues from
the operative field such as interposition or overlap,
lighting, outline and texture.1 The effect of reduction
in depth cues can be inferred from performance
differences under different viewing conditions, as
3D video systems that restore stereoscopic vision are
currently available.
Impaired hand-eye coordination:
The main variables
are the location of the monitor, degree of amplification,
mirrored movement and misorientation.2
Motion limitation:
The trocar restricts movement by
acting as invariant points.3 The surgeon´s dexterity
is affected because the range of motion is reduced to
four degrees of freedom compared to six needed to
perform free motion.
This movement restriction leads
to increased physical discomfort.
Reduction of haptic feedback:
The role of haptic feedback
is of special interest because it is used in important
decision-making scenarios such as the discrimination
of healthy versus abnormal tissues, identification of
organs and motor control. In laparoscopic surgery, it is
reduced but not absent as in robotic surgery.4-5
Vision is dependent on the cleanliness of laparoscopic optic, intra-abdominal smoke and light absorption:
Irrigation, blood, organic fluids, intra-abdominal
pressure and smoke can impair surgeon vision.The
irrigation of the operative field should be minimal as
the mixture of blood with serum alters light absorption
creating difficulties to discriminate structures and
surgical planes. Equilibrium is necessary between smoke
evacuation and pneumoperitoneum preservation.
ImAGInG dEVIcES
Minimally invasive surgery resulted from the introduction
of new imaging devices at look to internal organs through
pericentimetric or shorter incisions.
Surgical scopes ar
recognized as very old medical instruments conceived
many centuries ago when simple hollow tubes were used
to observe intracorporeal cavities.
Philip Bozzini in 1805
used the first illuminated scope consisted in a viewing
tube with a series of mirrors which reflected light from a
burning wax candle.
However, only in the 20th century, a
light scope was used to perform a diagnostic laparoscopy
and only after the success obtained with laparoscopic
cholecystectomies (1986), the medical industry started to
develop better imaging and optical devices.6
Although the skepticism of some during the years, today
we are facing a rapid advancement of minimally invasive
surgery in different disciplines and pathologies, and in
parallel, new imaging devices are appearing.
The surgeon
must be familiar with these developments.
سوزن گیر اپل apple
Laparoscope:
Traditionally, the laparoscope is a rigid
endoscope which is made of an outer ring of optical fibers,
used to transmit light into the abdominal and pelvic cavity
and an inner core of rod lenses via which the illuminated
operative field is captured by a camera.
Digital imaging
chips located within the camera allow the image from the
scope to be transmitted to an external display.
Various different types of laparoscope are available,
specified in terms of overall length, number of rods,
diameter and angle of view.
The diameter of laparoscopes
varies from 3 mm to 12 mm and the objective located
at the distal end offers an angle of view from 0 to 120
degrees. The brightness of the image is lower in thinner
scopes, due to less light transmission through the central
channel lenses.
However, with the improvement in the
optical fiber technology, even laparoscopes with 3 mm
of diameter are able to produce brighter and clearer
images.
The “angle of view” enables the operator to see
objects that might otherwise be out of camera view. A 30º
telescope provides a total field of view of 152º enabling
the visualization of the anterior abdominal wall and
working around masses or within deeper spaces.
A 0º
telescope provides a field of view of 76º, but offers a
panoramic view and more usual perspective (Fig. 1).
There is a laparoscope
model that has the possibility of
changing the view angle from 0° to 120º (Fig. 2). Flexible
tip laparoscopes are also available.
In gynecology, telescopes without instrument channels
are used in the majority of cases, as they give a better
overview and offer better image resolution.
However, in
some cases, it may be useful to use telescopes with an
integrated instrument channel (Fig. 3).
These laparoscopes
are generally 0º straightforward scopes. The diameter of
the instrument channel is 5–7 mm; thus, a correspondingly
large instrument can be inserted. CO2 laser can also be
connected to this laparoscope











نقد و بررسیها
هنوز بررسیای ثبت نشده است.