


رترکتور هوهمان بلانت
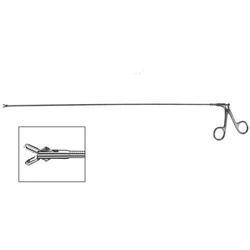
رترکتور هوهمان بلانت ( Blunt hohmann retractor ) :
دارای دسته مسطح با دو سوراخ در انتهای پروگزیمال خود می باشد .
دارای تیغه بلانت ، بسیار باریک و اندکی کرو است . این نوع رترکتور ، نیازی به اعمال کشش ندارد ، هنگامی که لبه آن در جای مورد نظر قرار گرفت ، کافی است دسته آن را به راحتی پایین یا عقب نگه دارید .
برای مشاهده صفحه اینستاگرام مامایی می توانید بر روی این لینک کلیک نمائید .
برای مشاهده و خرید انواع ابزار های جراحی عمومی می توانید بر روی این لینک کلیک نمائید .

Blunt hohmann retractor
مورد استفاده :
جهت کنار زدن حجم کمی از بافت در نواحی بسیار تنگ ، به کار می رود .
برای مشاهده محصولات دیگر برروی کلمه ی “ورودبه سایت“ کلیک نمایید./
-Click on the “Login to site“ to view other products. /
Preface
The third edition of the Essentials of Orthopedic Surgery provides a concise overview of orthopedic surgery directed toward third- and fourthyear medical students.
In this edition, physical diagnosis is a subsection in each chapter, which we believe gives better continuity.
Additionally, at the end of each chapter we have created a number of multiple-choice questions considered appropriate for medical students to be able to answer.
Each chapter has been revised to reflect updated material and, as in previous editions, we have kept to a standardized format as much as possible.
The topics are presented from a straightforward practical point-ofview, with the material being condensed to its most salient features.
Algorithms are at the heart of each chapter, with the decision points being based on practice standards and guidelines.
This format allows the student, when confronted with a specifi c clinical problem, to formulate both a diagnostic plan and a treatment plan.
Also, we have enjoyed working with our new publisher—Springer—and with Robert Albano as well as Sadie Forrester, who have guided this text to publication.
Finally, and most importantly, it has been again a very exciting and stimulating experience to work with all the members of the Department of Orthopaedics of Georgetown University Medical Center.
Since the last edition we have welcomed seven new members to the faculty, each a subspecialist.
Everyone has given very generously of their time.
We are most appreciative of each contribution and are proud of the final text.
tendon in chronic or massive rotator cuff tears Contraindications
1. Active soft tissue or glenohumeral infection
2. Neuropathic joint
3. Chronic axillary nerve injury
4. Failed prior surgical treatment with associated deltoid insufficiency (relative)
5. Degenerative arthritis (relative); consider combining rotator cuff repair with shoulder arthroplasty
6. Patient’s overall medical condition (relative)
7. Parkinson’s disease or other diseases that cause uncontrolled muscle activity (relative)
8. Patient unable to comply with postoperative
Contributors
xi Alan D. Aaron, MD†
Associate Professor, Department of Orthopaedic Surgery, Georgetown
University Medical Center, Washington, DC 20007, USA
Raymond M. Carroll, MD
Assistant Professor, Department of Orthopaedic Surgery, Georgetown
University Medical Center, Washington, DC 20007, USA
Paul S. Cooper, MD
Associate Professor, Department of Orthopaedic Surgery, Georgetown
University Medical Center, Washington, DC 20007, USA
John N. Delahay, MD
Peter and Rose Rizzo Professor and Vice Chairman, Department of
Orthopaedic Surgery, Georgetown University Medical Center, Washington, DC 20007, USA
Brian G. Evans, MD
Associate Professor and Vice Chairman for Operations and Finance,
Department of Orthopaedic Surgery, Georgetown University Medical
Center, Washington, DC 20007, USA
Mustafa A. Haque, MD
Assistant Professor, Department of Orthopaedic Surgery, Georgetown
University Medical Center, Washington, DC 20007, USA
Kristen Kellar-Graney, BS
Graduate Student, Interdisciplinary Tumor Biology Tra
Basic Science of Bone and Cartilage Metabolism
John N. Delahay
Normal Bone Growth and Development Bone is a biphasic connective tissue consisting of an inorganic mineral phase and an organic matrix phase.
The hardness of bone allows it to provide several specialized mechanical functions:
the protection of internal organs, the scaffold that provides points of attachment for other structural elements, and the levers needed to improve the efficiency of muscle action.
In addition, bone serves two biologic functions:
a site for hematopoietic activity and a reservoir of minerals needed for metabolic interchange.
Embryology The major components of the musculoskeletal system originate from the mesoderm layer of the trilaminar embryo.
This “middle layer” is populated by mesenchymal cells that are totipotent and capable of differentiating into a number of tissues.
The sequence of events important in bone growth and development begins with the appearance of the limb bud around the fifth week of life.
It is at that time that a tubular condensation of mesenchyme develops centrally in the limb bud.
Discrete areas, called interzones, are seen between these condensations (Fig. 1-1) and represent the primitive joints.
During the sixth week, the mesenchyme differentiates into cartilage through the process of chondrification (Fig. 1-2).
Interstitial and appositional growth occurs from within and from the surface, respectively.
In the seventh week, the cartilage model is penetrated by a vascular spindle, which occurs coincidentally with the necrosis of the central cartilage cells.
Once this vascular spindle is established, the central portion of the model is populated by osteoblasts.
Matrix is secreted and this in turn is ossified, making immature (woven) bone.














نقد و بررسیها
هنوز بررسیای ثبت نشده است.