





گراسپر روده ای هانتر
نام وسیله : گراسپر روده ای هانتر ( Hunter bowel grasper )
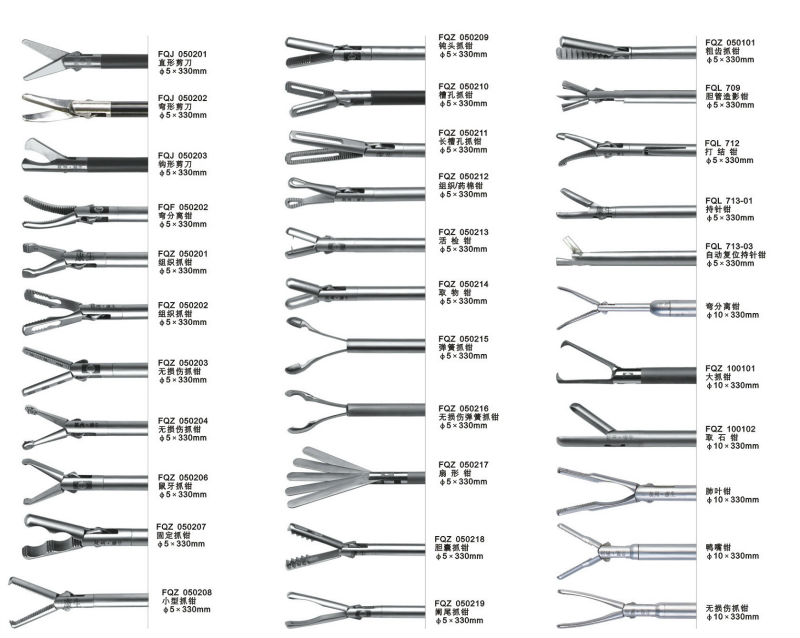
گراسپر روده ای هانتر ( Hunterbowel grasper ) :دارای آرواره های ظریف و بلند و شیارهای دی با کی شکل ( شیار های طولی هستند ) .
مورد استفاده : جهت گرفتن و جا به جایی اتروماتیک بافت های ظریف ( مثل روده و معده ) کاربرد دارد.
برای مشاهده محصولات دیگر برروی کلمه ی “ورودبه سایت“ کلیک نمایید./
–-Click on the “Login to site“ to view other products. /

Hunter bowel grasper
برای مشاهده ی صفحه ی اینستاگرام ما می توانید بر روی این لینک کلیک نمایید.
گراسپر روده ای هانتر Hunter bowel grasper
HY SHOULD WE DO LAPAROSCOPIC SURGERY?
The answer is simple: because patients can and do benefit from it. As long as the evidence suggests- and there is ample data by now- that laparoscopy has its benefits, it can be justified to be performed in various procedures.
Laparoscopic
cholecystectomy has replaced the traditional open approach to non-complicated gallbladder disease as the new gold standard because it results in less postoperative pain, less postoperative pulmonary dysfunction, faster return of bowel function, shorter length of hospital stay, faster return to normal
activities and work, and greater patient satisfaction.
These benefits also generally extend to other laparoscopic procedures.The advantages mentioned above result from the most obvious difference between laparoscopic and open surgery- that of less surgical trauma to the wound in laparoscopy. The access scar is minimized, leading to less pain, less wound infection and dehiscence, and better cosmetic result.
In addition, laparoscopy
also reduces tissue trauma during dissection, and subsequent blood loss, reduces systemic and immune response, and reduces adhesive complications.
From the surgeon’s point of view, the projected image on the monitor is a magnified image, resulting in better definition of structures.
It’s faster to close smaller wounds. And the recorded procedure can be used for review and training purposes. As in all surgical techniques and technologies, minimally invasive surgery also has its limitations and disadvantages. First, there may be problems encountered during access into the
abdominal cavity, such as iatrogenic injuries to the bowel or major vascular structures.
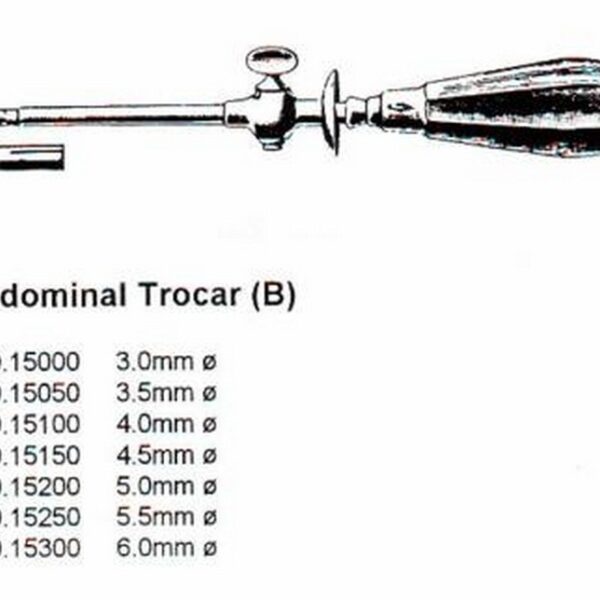
The incidence is about 0.05 to 0.1%. This incidence is reduced by practicing the open technique of introduction, rather than using the “blind” Veress needle technique, and using blunt-tipped trocars. Second, there may be undesirable side-effects of the carbon-dioxide pneumoperitoneum, such as hypercarbia, etc (see chapter on physiology of neumoperitoneum).
And third, from the surgeon’s perspective, the migration from open to laparoscopic skills means Introduction that the 3D vision is reduced to onocular 2D vision on the screen, depth perception and field of view is much reduced, and haptics, or the “feel” and tactile sensation of tissues, is limited to ross probing of tissues.
However, these limitations, once understood
and overcome have not hampered the development of laparoscopy. In a way, the surgeon is required to master a new set of skills to perform aparoscopy safely. With training and experience, surgery can be performed at a new standard that benefits patients.
IS WHICH TYPES OF SURGERY IS LAPAROSCOPY APPLICABLE?
Laparoscopy can now be performed in three main areas
of the body- the abdomen, the thorax, and closed spaces.
Laparoscopy can be used to resect tissues or to reconstruct tissues.
In the abdomen, we group laparoscopic techniques
according to major systems, as shown below.
a)
Gastrointestinal tract
– Laparoscopic-assisted oesophagectomy
– Laparoscopic cardiomyotomy for achalasia
– Laparoscopic fundoplication for gastro-oesophageal
reflux disease
– Laparoscopic bariatric surgery (banding, bypass) for
morbid obesity
– Laparoscopic gastrectomy and small bowel procedures
– Laparoscopic appendicectomy
– Laparoscopic colectomy
– Laparoscopic adhesiolysis and diagnostic laparoscopy
b)
Hepato-biliary-pancreatic system
– Laparoscopic cholecystectomy
– Laparoscopic liver and bile duct procedures
– Laparoscopic management of pseudocysts and
pancreatic procedures
Introduction
– Laparoscopic bypass procedures
– Laparoscopic splenectomy
c)
Endocrine system
– Laparoscopic adrenalectomy
– Laparoscopic enucleation of benign pancreatic islet
tumours
– Endoscopic Neck Surgery
d)
Abdominal Wall
– Laparoscopic inguinal hernia repair
– Laparoscopic repair of incisional hernia
e)
Urologic system
– Laparoscopic nephrectomy
– Laparoscopic procedures for ureteric and bladder
conditions
f)
Gynecology
– Laparoscopic management of tubo-ovarian conditions
– Laparoscopic hysterectomy
In the thorax, some procedures include,
– Thoracoscopic sympathectomy for palmar
hyperhidrosis
– Thoracoscopic pleurodesis
– Thoracoscopic bullectomy and partial lobectomy
With the use of novel devices, adequate operating space can
be created in “closed” spaces so that endoscopic techniques
can be performed, such as,
– Endoscopic extraperitoneal inguinal hernia repair
– Endoscopic ligation of saphenous venous perforators
in the leg
– Endoscopic approach to neck organ such as the thyroid
and parathyroid glands
Introduction
One can see that laparoscopy is
widely applied. It’s important,however, to realize that for certain conditions, laparoscopy is
feasible but does not necessarily replace open techniques. The
practice will depend on the expertise available and also on
literature evidence that laparoscopy is superior to the open
approach.
TRAINING ISSUES
Surgical training is the core reason for the conception of
this training manual. Surgeons in training are taught well
established skills in open surgery.
However, learning of
laparoscopic skills is now becoming an increasingly important part
of the training program because of the new set of skills that need
to be acquired. The main focus is to operate efficiently and
minimize surgical errors, i.e. operate safely.
Training and constant
practice are ways to overcome the learning curve. A case point
is the dramatic increase by three to five fold in bile duct injuries in
the early years when laparoscopic cholecystectomy was
performed by inexperienced and poorly trained surgeons; the
rate has since dropped to acceptable levels.
Effective teaching and learning involves dedicated staff with experience in laparoscopic surgery who are good educators and enthusiastic students who are keen to acquire new knowledge and skills.
This is facilitated by modern teaching instruments such as laparoscopic trainers, virtual simulators, CDROMs, the Internet, and software programs, all available in the in-house skills lab in the Minimally Invasive Surgical Centre (MISC).
In addition to these activities, meetings and workshops all contribute to CME activities. Training programs comprise of two broad categories- Basic
and Advanced Laparoscopic skills.
In the basic program, the student is taught about familiarization with equipment and instruments, physiology of pneumoperitoneum, access and port
placements, diathermy and dissection techniques, and safety issues.
This is extended in the advanced program to suturing skills, use of instruments in advanced techniques, and familiarization with advanced procedures. The training program at the MISC, IntroductionNUH runs twice yearly. Each course has four modules that total 12 hours of training.
THE FUTURE OF MINIMALLY INVASIVE SURGERY
Minimally invasive surgery, as it stands today, has been the result of intense and continuous development and innovation on the part of surgeons in echniques, private industries in instrumentation, and in no small part by public demands and patient requests.
Surgical innovation will and should continue,however, while maintaining a balance of not escalating costs of healthcare delivery.
The progress of MIS will mirror that of developments in instrumentation, because technical innovation and expansion into previously “difficult” erritories and advanced procedures has reached a plateau.
With better and newer instruments, procedures can be performed faster and more effectively, with the potential of reducing operating duration and verall costs.
With progress in information technology (IT), mass data can be exchanged faster along the Internet and ISDN lines, thus enabling more use of eletransmission and teleproctoring to remote areas.
Robotic devices have been developed to assist in surgery and may one day also allow surgeons to operate from remote locations. And interconnectivity of information will streamline the process of surgery.
In conclusion, laparoscopy is a marriage of surgical skills, surgical innovation, and technology advancements.
Training is at the core of improving the performance of surgeons so that patients benefit from the high quality of care given to them.
TECHNICAL CONSIDERATIONS
OPERATING ROOM SET-UP:
The proper hardware and instruments are essential for performing
a safe laparoscopy.
Most large medical centers have one or several dedicated interventional laparoscopic operating rooms.There should be a sufficient back up of strumentation to cover for equipment failure. Using an electric or powered operating room table is a definite asset.
In most cases, the surgeon has to frequently change the position of the patient in order to enhance exposure and visualization. If performing aparoscopic bariatric procedures, the weight limit of the operating room table should be checked.
Computer-ready-connected operating table are a must if the surgical team uses a surgical robot.In addition facilities for intra-operative imaging should be available.
grasper















نقد و بررسیها
هنوز بررسیای ثبت نشده است.