


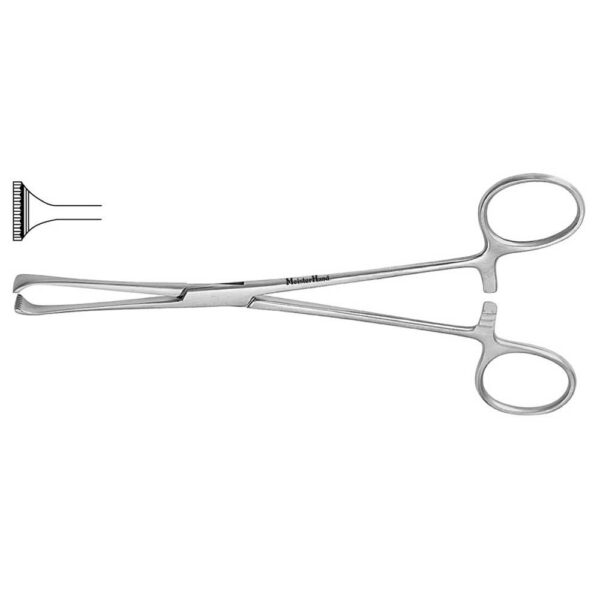
انبر قفل دار جراحی
pliers انبر قفل دار جراحی ( channel locks ) : دارای دسته های سینگل – اکشن با آرواره های درارای دندانه های ضخیم بانوک راند ، می باشد .
لولای آن ، دو زاویه باز شدن را برای آرواره ها فراهم می آورد .
مورد استفاده انبر قفل دار جراحی :
جهت گذاشتن یا خارج کردن سخت افزار ها و نگه داشتن نوک تروکار ها در طول گذاشتن درون زخم های عمیق ، کار برد دارد .
برای مشاهده و خرید انواع ابزار های جراحی عمومی می توانید بر روی این لینک کلیک نمائید .
، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ،، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ، ،
برای مشاهده صفحه اینستاگرام مامایی می توانید بر روی این لینک کلیک نمائید .

channel locks
برای مشاهده محصولات دیگر برروی کلمه ی “ورودبه سایت“ کلیک نمایید./
–-Click on the “Login to site“ to view other products. /
Indications (Rotator Cuff Repair)
1. Patients with chronic shoulder pain or weakness with a documented rotator cuff tear that has failed nonsurgical management (rest, local modalities, NSAIDs, physical therapy, and judicious subacromial cortisone injections)
2. Acute, traumatic full-thickness rotator cuff tears
3. Partial-thickness rotator cuff tears greater than 50% Indications for associated acromioclavicular (AC) joint resection
➣ AC joint tenderness on physical examination
➣ Radiographic changes of AC joint arthritis
➣ Exposure optimization of a retracted supraspinatus
tendon in chronic or massive rotator cuff tears Contraindications
1. Active soft tissue or glenohumeral infection
2. Neuropathic joint
3. Chronic axillary nerve injury
4. Failed prior surgical treatment with associated deltoid insufficiency (relative)
5. Degenerative arthritis (relative); consider combining rotator cuff repair with shoulder arthroplasty
6. Patient’s overall medical condition (relative)
7. Parkinson’s disease or other diseases that cause uncontrolled muscle activity (relative)
8. Patient unable to comply with postoperative
rehabilitation Preoperative Preparation
1. Physical examination to include assessment of AC joint tenderness and/or pain with shoulder adduction
2. Obtain radiographs a. Anteroposterior (AP) in plane of scapula (true AP)
b. AP shoulder (check distal clavicle for “spurs”)
c. Axillary view (check for os acromiale, glenohumeral arthritis)
d. Supraspinatus outlet view (assess acromion shape [types I–III], spinoacromial angle)
e. 25 degree caudal tilt (“Rockwood view”) (optional)
3. Consider magnetic resonance imaging (MRI): helps evaluate extent (“full” versus “partial” thickness)
of rotator cuff tears, and presence of muscle atrophy or tendon retraction; observe mass effect of acromion and AC joint on supraspinatus tendon (impingement).
Special Instruments, Position, and Anesthesia













نقد و بررسیها
هنوز بررسیای ثبت نشده است.